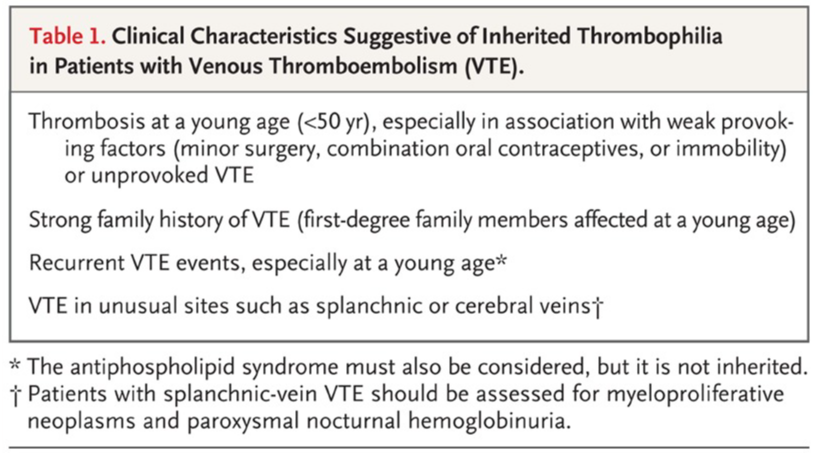
Deciding who should get thrombophilia tests and how to interpret the results is complex. The clinical benefits of testing and its impact on venous thromboembolism (VTE) management are unknown. Some clinical findings can indicate inherited thrombophilia, such as VTE at a young age, strong family history, recurrent VTE, or VTE in unusual sites. However, age and family history should be carefully considered.
Testing for inherited thrombophilia is controversial due to its limited effect on VTE outcomes, including death. Positive results may lead to unnecessary overtreatment, while negative results can falsely reassure patients and providers. Moreover, potential for misdiagnosis because current tests may not capture all cases of inherited thrombophilia.
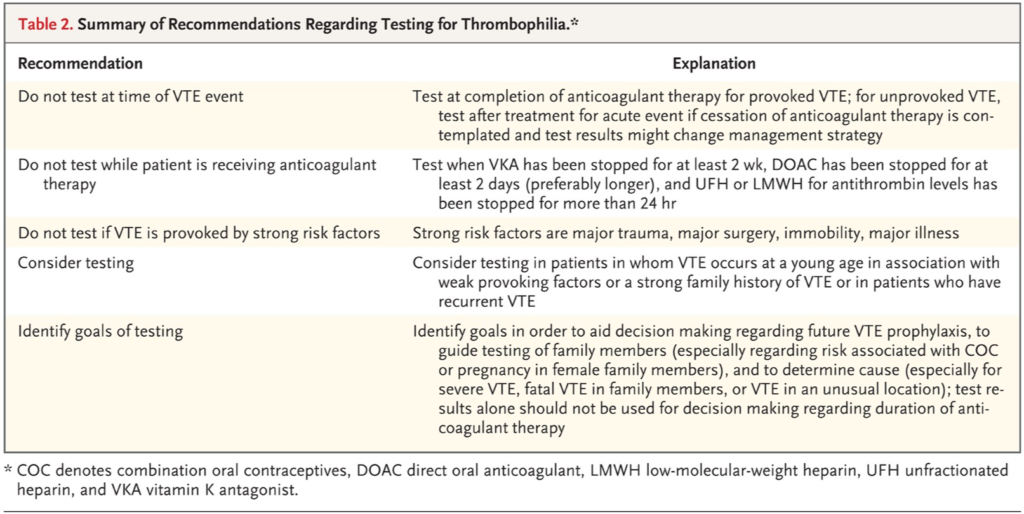
In patients with acute VTE, thrombophilia testing is not necessary during initial presentation, as full-intensity anticoagulant therapy is required regardless of the cause. Acute conditions can affect test results, leading to uncertainty and increased costs. Therefore, testing for thrombophilia during hospitalization for acute VTE is unnecessary as it does not change the initial management.
Thrombophilia Testing
Thrombophilia testing do not significantly impact the management of venous thromboembolism (VTE). The decision to test a patient should be based on how the results will be used, as they should not influence decisions about the duration of anticoagulant therapy for VTE management. Positive results may reinforce adherence to prophylaxis, but negative results do not necessarily indicate low risk.
While thrombophilia status may be considered when making decisions about secondary prophylaxis after a first provoked VTE or primary prophylaxis for positive family members at times of increased risk, the supporting data for such practices are limited. There is no evidence suggesting that patients with an inherited thrombophilia or VTE should be treated differently from patients without thrombophilia.
The accuracy of the test will depend on the completion of anticoagulant therapy and discontinuation of oral anticoagulants for a certain period of time. If the risk of recurrent VTE is too high to stop anticoagulant therapy, testing for thrombophilia may not be helpful in guiding patient care. Antiphospholipid antibodies should not be assessed when VTE is clearly provoked by surgery or other high-risk events.
Thrombophilia Tests
Thrombophilia tests are used to assess the risk of developing venous thromboembolism (VTE). The tests focus on factors associated with heritable VTE risks, including deficiencies of natural anticoagulants (protein S, protein C, and antithrombin) and specific gene mutations (factor V Leiden and prothrombin gene mutation). Some tests, such as elevated factor VIII, IX, XI activity, and plasminogen activator inhibitor type 1 (PAI-1) level, have not conclusively shown an association with VTE risk and require further validation. Additionally, inherited thrombophilias do not appear to contribute significantly to arterial thrombotic events, so these tests should not be ordered for evaluating myocardial infarction, stroke, or peripheral arterial thrombosis.
For the diagnosis of antiphospholipid syndrome, which involves both arterial and venous thrombosis, tests for antiphospholipid antibodies are important. These include clot-based assays for lupus anticoagulants and ELISA-based tests for IgG and IgM anticardiolipin antibodies and IgG and IgM anti–beta-2 glycoprotein 1 antibodies. The diagnosis of lupus anticoagulant syndrome requires meeting both clinical and laboratory criteria, with positive test results being persistently positive on two occasions at least 12 weeks apart. The presence of antiphospholipid antibodies alone does not confirm the diagnosis of antiphospholipid syndrome. Adherence to strict diagnostic criteria is essential for appropriate patient care.
Approach to VTE Management
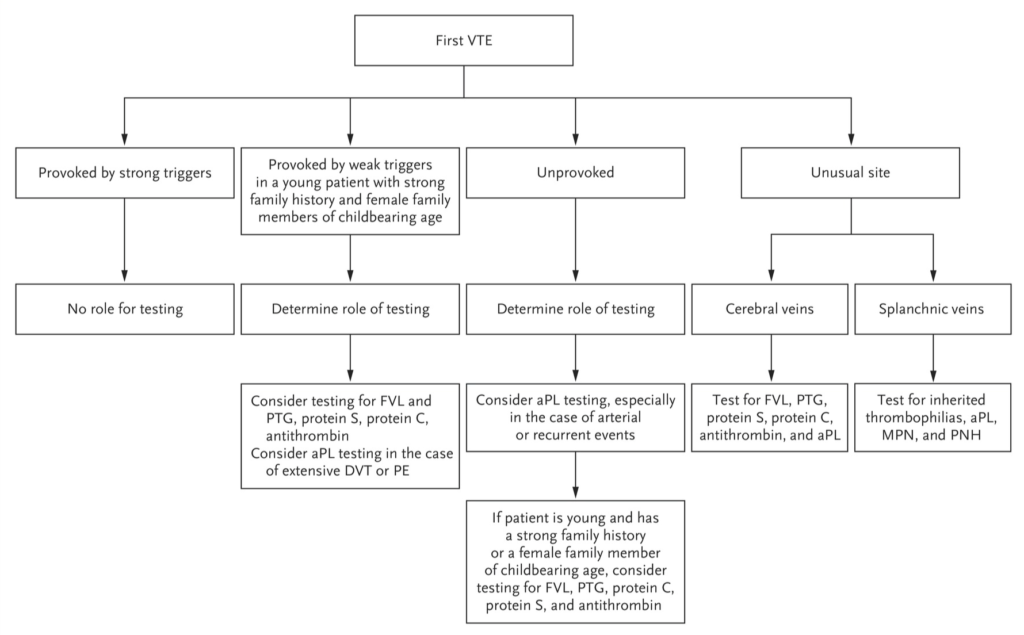
The management of venous thromboembolism (VTE) involves determining the duration of anticoagulant therapy based on whether the VTE was provoked or unprovoked. Thrombophilia status has limited influence on this decision-making process. Provoked VTE events, caused by strong transient factors like surgery, trauma, or immobility, generally have a low risk of recurrence regardless of thrombophilia status. Patients with provoked VTE usually do not require lifelong anticoagulation, even if they have inherited thrombophilia.
In contrast, patients with unprovoked VTE face a significantly higher risk of recurrence after stopping anticoagulant therapy. However, the presence of common inherited thrombophilias like factor V Leiden or the prothrombin gene mutation does not influence the risk of recurrence in these cases. Unprovoked VTE patients with inherited thrombophilia do not require lifelong anticoagulation either, as their recurrence risk is not substantially higher than those without inherited thrombophilia. Antiphospholipid antibody testing might be useful in cases of first, unprovoked VTE when there is uncertainty about stopping anticoagulant therapy. Positive results, along with appropriate clinical criteria, could impact management decisions. Overall, the risk of recurrence and the type of VTE (provoked or unprovoked) are more crucial in determining the duration of anticoagulation than thrombophilia status.
Special Situations
Special situations in the management of venous thromboembolism (VTE) involve specific factors that may influence the approach to treatment:
- Antiphospholipid Syndrome: This acquired thrombophilia is associated with both venous and arterial thrombosis and generally confers a high risk of recurrent VTE. Patients with clinically significant, unprovoked thrombotic events and persistently high levels of antiphospholipid antibodies may require continued anticoagulant therapy.
- Thrombosis in Unusual Locations: VTE occurring in splanchnic-veins (portal, hepatic, splenic, or mesenteric) and cerebral veins is less common and requires careful management. While inherited thrombophilias may be associated with an increased risk of VTE in these sites, screening for thrombophilia has not been shown to play a role in their care.
- High-Estrogen States: Estrogen-containing contraceptives are associated with an increased risk of VTE, particularly in women with inherited thrombophilias. For young female patients considering estrogen use, testing for thrombophilia may provide guidance in contraceptive choices. However, a negative family history of VTE with positive thrombophilia results does not indicate a low risk of VTE. Pregnancy-related VTE management should not change based on thrombophilia status, and antepartum prophylaxis for women with inherited thrombophilia is controversial.
- Cancer-Related Thrombosis: Patients with cancer, especially mucin-producing adenocarcinomas, have an increased risk of VTE. While inherited thrombophilia adds to the risk, management of VTE in cancer patients is not influenced by thrombophilia status, and testing is unnecessary.
Overall, the management of VTE in these special situations is primarily based on clinical factors and risk assessment, rather than thrombophilia status.
Conclusion
The development of venous thromboembolism (VTE) involves both genetic and environmental factors. Patients with inherited thrombophilia have a higher relative risk of experiencing a first VTE, but the risk of recurrent VTE is similar to those without inherited thrombophilia. The presence of antiphospholipid antibodies, an acquired thrombophilia, requires careful assessment to determine the need for prolonged anticoagulant therapy and the diagnosis of antiphospholipid syndrome. Thrombophilia testing should be done cautiously, considering its limitations and appropriate patient selection, and using the results based on available data to provide the best care for VTE patients.
The full journal can be found on the NEJM website: https://www.nejm.org/doi/10.1056/NEJMra1700365
Reference:
- Thrombophilia Testing and Venous Thrombosis” published in the New England Journal of Medicine: Connors JM. Thrombophilia Testing and Venous Thrombosis. N Engl J Med. 2017;377(11):1177-1187. doi:10.1056/NEJMra1700365
Leave a Reply