
Background:
Treatment-resistant depression is a severe condition with limited treatment options. Conventional antidepressants often have diminishing efficacy with each successive course of treatment, leading to significant challenges in managing this condition. Psilocybin, a compound found in certain mushrooms, has shown promise as a potential antidepressant in preliminary studies, particularly in patients with life-threatening illnesses. This phase 2 clinical trial aimed to determine the efficacy and safety of synthetic psilocybin (COMP360) in patients with treatment-resistant major depressive episodes.
Summary:
In this phase 2 double-blind clinical trial, 233 participants with treatment-resistant major depression received a single dose of psilocybin (25 mg, 10 mg, or 1 mg control). The primary endpoint was the change in Montgomery–Åsberg Depression Rating Scale (MADRS) total score from baseline to 3 weeks. Results showed that the 25 mg dose significantly reduced MADRS scores compared to the 1 mg dose, while the 10 mg dose did not show significant improvement. Response rates at week 3 were 37% in the 25 mg group, 19% in the 10 mg group, and 18% in the 1 mg group. Remission rates were 29% in the 25 mg group, 9% in the 10 mg group, and 8% in the 1 mg group. The study emphasized the need for clinical vigilance regarding suicidality in future psilocybin trials for depression.
Endpoints:
- Primary Endpoint: Change in MADRS total score from baseline to 3 weeks.
- Secondary Endpoints: Response (≥50% decrease in MADRS score at week 3), Remission (MADRS score ≤10 at week 3), and Sustained Response (maintained response from week 3 to week 12).
Analysis:
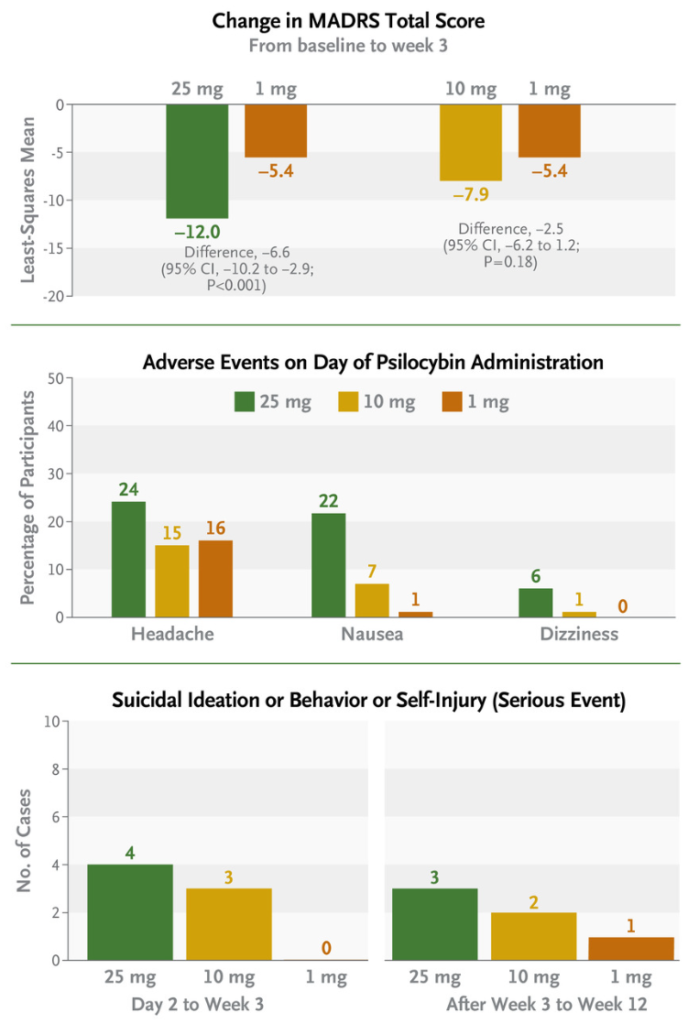
The study was well-structured, with multiple safety assessments throughout the trial. Adverse events, including headache, nausea, and dizziness, were more common in the 25 mg and 10 mg groups, but no serious adverse events occurred on the day of psilocybin administration. However, some participants in the higher-dose groups experienced suicidal ideation and self-injurious behavior, emphasizing the need for vigilance in future trials. The study acknowledges limitations such as the lack of an active comparator and the exclusion of high suicide risk individuals.
Results:
- Primary Efficacy End Point (Change in MADRS Total Score at Week 3):
- Change from baseline to week 3 in the MADRS total score:
- 25-mg group: -12.0 points
- 10-mg group: -7.9 points
- 1-mg group: -5.4 points
- Difference in change between the 25-mg group and the 1-mg group: -6.6 points
- Difference in change between the 10-mg group and the 1-mg group: -2.5 points
- Change from baseline to week 3 in the MADRS total score:
- Response Rates at Week 3:
- 25-mg group: 37%
- 10-mg group: 19%
- 1-mg group: 18%
- Remission Rates at Week 3:
- 25-mg group: 29%
- 10-mg group: 9%
- 1-mg group: 8%
- Sustained Response Rates at Week 12:
- 25-mg group: 20%
- 10-mg group: 5%
- 1-mg group: 10%
- Adverse Events (Overall Incidence):
- 25-mg group: 84%
- 10-mg group: 75%
- 1-mg group: 72%
- Adverse Events on the Day of Psilocybin Administration (Day 1):
- Headache (25-mg group): 24%
- Nausea (25-mg group): 22%
- Dizziness (25-mg group): 6%
- Fatigue (25-mg group): 6%
- Severe Adverse Events After Week 3 (End of Trial):
- 25-mg group: 3%
- 10-mg group: 4%
- 1-mg group: 0%
- Baseline Suicidal Ideation:
- 25-mg group: 27%
- 10-mg group: 36%
- 1-mg group: 24%
- Participants with Worsening Suicidal State from Baseline to Week 3:
- 25-mg group: 14%
- 10-mg group: 17%
- 1-mg group: 9%
Statistical Analysis:
- Change from baseline to week 3 in the MADRS total score:
- This indicates the difference in the severity of depressive symptoms from the baseline (initial assessment) to week 3 of treatment.
- In the 25-mg group, on average, participants experienced a reduction of 12.0 points in their MADRS (Montgomery-Åsberg Depression Rating Scale) total score during this time.
- In the 10-mg group, the reduction was 7.9 points.
- In the 1-mg group, the reduction was 5.4 points.
- These values reflect how effective the treatment was in reducing depressive symptoms. A greater reduction indicates better improvement.
- Difference in least-squares mean change between 25-mg and 1-mg groups:
- This statistic compares the change in MADRS total score specifically between the 25-mg group and the 1-mg group.
- The difference was -6.6 points, meaning that, on average, participants in the 25-mg group had a 6.6 point greater reduction in depressive symptoms compared to those in the 1-mg group.
- The 95% confidence interval (CI) indicates the range within which we can be reasonably confident the true difference lies. In this case, it’s -10.2 to -2.9.
- The “P<0.001” suggests that this difference is statistically significant, meaning it’s very unlikely to be due to chance.
- Odds ratio for response at week 3 (25-mg vs. 1-mg group):
- The odds ratio of 2.9 indicates that at week 3, participants in the 25-mg group were 2.9 times more likely to respond positively to treatment compared to those in the 1-mg group.
- 95% CI (1.2 to 6.6)
- Odds ratio for remission at week 3 (25-mg vs. 1-mg group):
- The odds ratio of 4.8 indicates that at week 3, participants in the 25-mg group were 4.8 times more likely to achieve remission (a state of being free from symptoms) compared to those in the 1-mg group.
- 95% CI (1.8 to 12.8)
- Odds ratio for sustained response at week 12 (25-mg vs. 1-mg group):
- The odds ratio of 2.2 indicates that at week 12, participants in the 25-mg group were 2.2 times more likely to maintain a positive response compared to those in the 1-mg group.
- 95% CI (0.9 to 5.4)
In summary, these statistics help evaluate the effectiveness of the different doses of psilocybin in treating depression. A lower MADRS score, a higher difference in MADRS score between groups, and higher odds ratios for response, remission, or sustained response all suggest a more favorable response to treatment. The confidence intervals provide a measure of uncertainty around these estimates.
Limitations:
- Lack of an active comparator.
- Limited ethnically diverse participant sample.
- Exclusion of high-risk individuals for suicide.
- Difficulty maintaining the double-blind structure due to the psychedelic effects of psilocybin.
- Uncertainty regarding the effects of different psilocybin preparations.
The study suggests that psilocybin, particularly at a 25 mg dose, may have potential as a treatment for treatment-resistant depression. However, further research with larger and longer trials, as well as comparisons with existing depression treatments, is needed to confirm its efficacy and safety.
Keywords: Psilocybin, treatment-resistant depression, clinical trial, Montgomery–Åsberg Depression Rating Scale, antidepressant, suicidal ideation.
Full research paper can be found on NEJM
Goodwin, G. M., Aaronson, S. T., Alvarez, O., et al. (2022). Single-dose psilocybin for a treatment-resistant episode of major depression. New England Journal of Medicine, 387(18), 1637-1648. doi:10.1056/NEJMoa2206443
Leave a Reply