Background
As the proportion of older patients (≥75 years of age) with myocardial infarction admitted to hospitals increases, the challenge of effective treatment in this demographic becomes apparent. However, older patients are often underrepresented in clinical trials, leading to a lack of robust evidence for their management. One particular challenge is deciding whether to pursue complete coronary-artery revascularization through percutaneous coronary intervention (PCI) in these patients. While the benefits of complete revascularization are well-established in younger patients with multivessel coronary artery disease, its advantages in older patients are uncertain. To address this gap in knowledge, the Functional Assessment in Elderly MI Patients with Multivessel Disease (FIRE) trial was conducted to investigate whether physiology-guided complete revascularization is superior to culprit-only PCI in older patients with myocardial infarction and multivessel disease.
What is difference between physiology guided complete revascularization and culprit-only PCI?
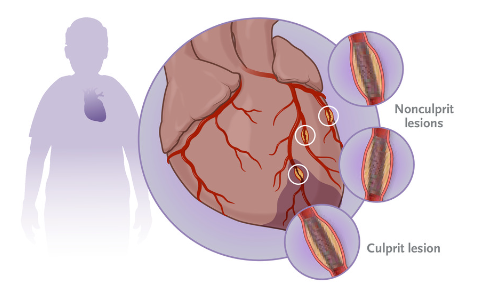
Physiology-Guided Complete Revascularization: In this approach, the focus is on treating all significant coronary artery blockages (lesions) beyond just the culprit lesion responsible for the heart attack. The decision to perform PCI on nonculprit lesions is guided by physiological measurements, such as fractional flow reserve (FFR) or other indices that assess the functional significance of the blockages. Lesions that are physiologically significant (i.e., causing reduced blood flow) are treated with PCI.
Culprit-Only PCI: This approach involves treating only the culprit lesion responsible for the MI. Nonculprit lesions, even if they have significant blockages, are not treated immediately. The primary goal is to restore blood flow to the heart muscle as quickly as possible by addressing the cause of the heart attack.
Methods
Trial Design and Oversight: The FIRE trial was a multicenter, prospective, randomized trial involving older patients (≥75 years) with ST-segment elevation myocardial infarction (STEMI) or non–ST-segment elevation myocardial infarction (NSTEMI) and multivessel disease. The trial was designed to evaluate physiology-guided complete revascularization compared to culprit-only revascularization.
Patients: Eligible patients had to be at least 75 years old, admitted with STEMI or NSTEMI, and have multivessel disease with a nonculprit lesion in a coronary artery with specific criteria. Exclusion criteria included an inability to identify a clear culprit lesion, localization of the nonculprit lesion in the left main coronary artery, planned or previous surgical revascularization, or a life expectancy of less than 1 year. All patients provided informed consent.
Randomization: After successful treatment of the culprit lesion, patients were randomized to receive either physiology-guided complete revascularization or culprit-only revascularization in a 1:1 ratio. Randomization was concealed through a Web-based system.
Treatments and Follow-up: Patients assigned to physiology-guided complete revascularization underwent PCI of all significant nonculprit lesions, guided by physiological and angiographic assessments. Guideline-based medical therapy was indicated for both groups, with dual antiplatelet therapy recommended for at least 1 year.
Results
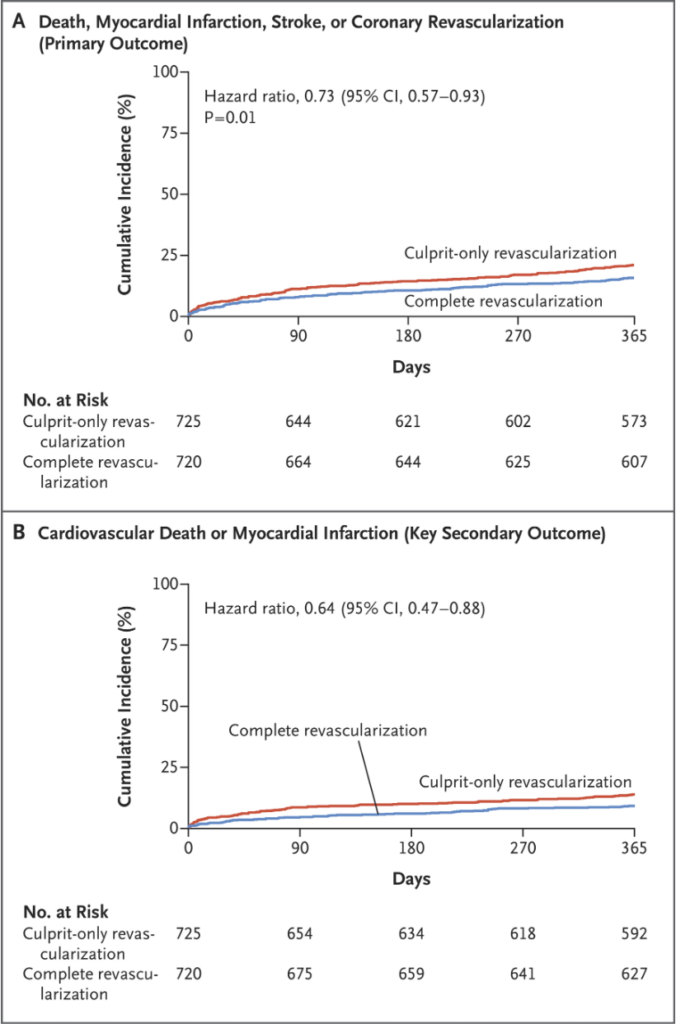
The primary outcome was a composite of death, myocardial infarction, stroke, or ischemia-driven coronary revascularization within 1 year. Key secondary outcomes included cardiovascular death or myocardial infarction at 1 year and individual components of the primary outcome. Safety outcomes included contrast-associated acute kidney injury, stroke, or bleeding.
Statistical Analysis: The trial was designed to provide 80% power to demonstrate the superiority of complete revascularization over culprit-only revascularization. Analyses were performed on an intention-to-treat basis, and hazard ratios with 95% confidence intervals were estimated. The statistical significance level was set at P<0.05.
Results: From July 18, 2019, to October 25, 2021, a total of 1898 patients were screened, with 1445 patients randomized to receive either complete or culprit-only revascularization. The median age was 80 years, and the majority of patients had STEMI. The primary outcome occurred in 15.7% of the complete-revascularization group and 21.0% of the culprit-only group, resulting in a hazard ratio of 0.73 (95% CI, 0.57 to 0.93, P=0.01). Secondary outcomes also favored complete revascularization.
In terms of safety, no significant difference was observed between the two treatment groups regarding the composite safety outcome, which included contrast-associated acute kidney injury, stroke, or bleeding (BARC type 3, 4, or 5). The incidence rates were 22.5% in the complete-revascularization group and 20.4% in the culprit-only group. The hazard ratio was 1.11, with a 95% confidence interval of 0.89 to 1.37, and the p-value was 0.37. This indicates that there was no statistically significant variation in safety outcomes between the two treatment approaches.
What is Hazard Ratio?
Hazard Ratios: These ratios measure the relative risk of an event occurring in one treatment group compared to another. A hazard ratio less than 1 indicates a lower risk in the first group. When the HR is greater than 1, it suggests that the group with the higher HR has a higher risk of experiencing the event being studied. In other words, there is an increased likelihood of the event happening in that group.
What is Confidence Interval?
Confidence Intervals (CIs): CIs provide a range of values within which the true effect size is likely to lie. A narrow CI indicates greater precision in the estimate. When the CI includes 1, it means that the observed HR is not statistically significantly different from 1. This suggests that the effect observed in the study is not statistically significant and may be due to random chance.
Discussion
The FIRE trial addressed the lack of evidence for revascularization strategies in older patients with myocardial infarction and multivessel disease. Physiology-guided complete revascularization was associated with a lower occurrence of the composite primary outcome, indicating its potential benefit in this population. The results provide valuable insights into the management of older patients with myocardial infarction.
Limitations
Keywords: myocardial infarction, older patients, complete revascularization, physiology-guided, PCI, outcomes, clinical trial.
The full Research paper can be found on NEJM.
Reference
Biscaglia, S., Guiducci, V., Escaned, J., Moreno, R., Lanzilotti, V., Santarelli, A., Cerrato, E., Sacchetta, G., Jurado-Roman, A., Menozzi, A., Amat Santos, I., Díez Gil, J. L., et al. (2023). Complete or culprit-only PCI in older patients with myocardial infarction. New England Journal of Medicine, 389(889-898), 10.1056/NEJMoa2300468.
Leave a Reply