
Background
Atrial fibrillation (A.Fib) can arise from various underlying causes that lead to changes in the structure of the heart. Patients with A.Fib have an increased risk of stroke due to blood clot formation in the left atrium. Clot can travel to the brain and cause a stroke. A.Fib is frequently linked to conditions like aging, ischemic heart disease, and hypertension. However, rheumatic heart disease is also associated with A.Fib in particular in low and middle income countries. Traditionally A.Fib is treated with anticoagulation therapy more commonly vitamin K antagonist such as Warfarin.
Summary
The article focuses on comparing the effectiveness of the factor Xa inhibitor rivaroxaban with vitamin K antagonist therapy (warfarin) for stroke prevention in patients with A.Fib and rheumatic heart disease. Randomized trials have previously demonstrated the efficacy of vitamin K antagonists for stroke prevention, but these drugs require regular monitoring and dietary considerations. Due to the strict regulations while being on the vitamin K antagonist this led to the development of direct thrombin inhibitors and factor Xa inhibitors like rivaroxaban which do not require as much monitoring. These newer agents have been proven to be effective for stroke prevention and have a reduced risk of intracranial bleeding.
Analysis
Patient Population and Trial Design
The study involved patients with documented rheumatic heart disease-associated A.Fib. The trial compared rivaroxaban to vitamin K antagonist therapy in a randomized manner. The trial protocol was approved by relevant authorities, and patients provided informed consent.
Patient Enrolment and Treatments
Patient inclusion criteria involved age, echocardiographically proven rheumatic heart disease, and documented A.Fib. Patients were randomized to receive either locally approved vitamin K antagnost or rivaroxaban. Dosing was based on creatinine clearance. Patients were followed up at various intervals.
Outcome Measures
Primary Efficacy
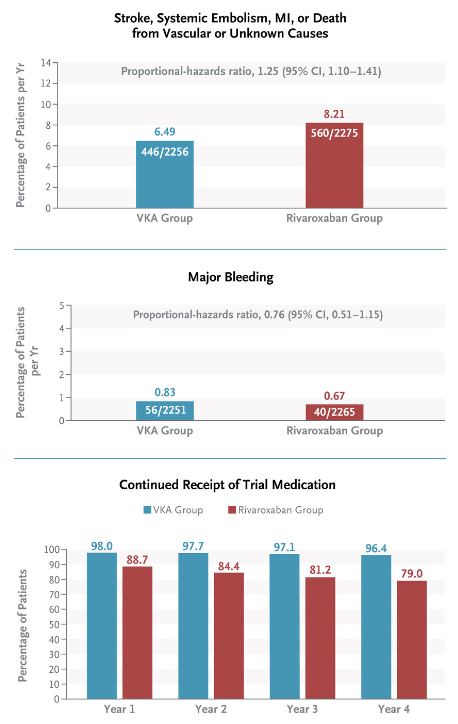
Composite of total stroke, systemic embolism, myocardial infarction, or death from vascular or unknown causes.
Secondary Efficacy
Myocardial infarction or death from vascular (cardiac or noncardiac) causes.
The trial was powered to continue until a specified number of primary outcomes occurred – 1079.
Results
Trial had a total of 4565 patients, with both treatment groups having comparable baseline characteristics. Hazard ratio of 1.25 was found in the rivaroxaban group indicating the group had a 25% higher likelihood of experiencing the primary outcome as compared to the comparison group.
A hazard ratio (HR) compares the risk of an event occurring between two groups in a survival analysis. Quantifies the relative likelihood of the event happening in one group compared to the other. HR greater than 1 indicates a higher risk in the first group, while a HR less than 1 suggests a lower risk.
The difference in restricted mean survival time between the two groups 1599 days in the rivaroxaban group and 1675 days in the vitamin K antagonist group was statistically significant, favoring vitamin K antagonist therapy. Mortality was significantly lower in the vitamin K antagonist group, and the causes of death differed between the groups.
Restricted mean survival time compares the average survival time between two groups in a study. A higher restricted mean survival time in one group suggests, on average, longer survival compared to the other group over the specified study period.
Discussion
The unexpected difference in mortality and stroke outcomes raised questions. Possible explanations included the trial’s reduced power for stroke outcomes due to lower-than-expected rates and a potential delay in the onset of benefits from vitamin K antagonist therapy. Adherence to rivaroxaban and its discontinuation may have contributed to the observed differences. The trial results also suggested a direct effect of vitamin K antagonists on rheumatic heart disease progression, as it led to a lower risk of vascular death.
Implications
This study highlights the significance of choosing appropriate anticoagulation therapy for patients with A.Fib and rheumatic heart disease. The results suggest that vitamin K antagonist therapy may have benefits beyond stroke prevention, influencing mortality and disease progression. It reinforces the importance of considering patient characteristics and underlying conditions when selecting anticoagulant treatments for atrial fibrillation.
The full Research paper can be found on NEJM
Reference
Connolly SJ, Karthikeyan G, Ntsekhe M, Haileamlak A, El Sayed A, El Ghamrawy A, Damasceno A, Avezum A, Dans AM, Gitura B, Hu D, Kamanzi ER, Maklady F, Fana G, Gonzalez-Hermosillo JA, Musuku J, Kazmi K, Zühlke L, Gondwe L, Ma C, Paniagua M, Ogah OS, Molefe-Baikai OJ, Lwabi P, Chillo P, Sharma SK, Cabral TJ, Tarhuni W, Benz A, van Eikels M, Krol A, Pattath D, Balasubramanian K, Rangarajan S, Ramasundarahettige C, Mayosi B, Yusuf S, on behalf of the INVICTUS Investigators. (2022). Rivaroxaban in rheumatic heart disease-associated atrial fibrillation. N Engl J Med. 387(11):978-988. doi:10.1056/NEJMoa2209051
Leave a Reply