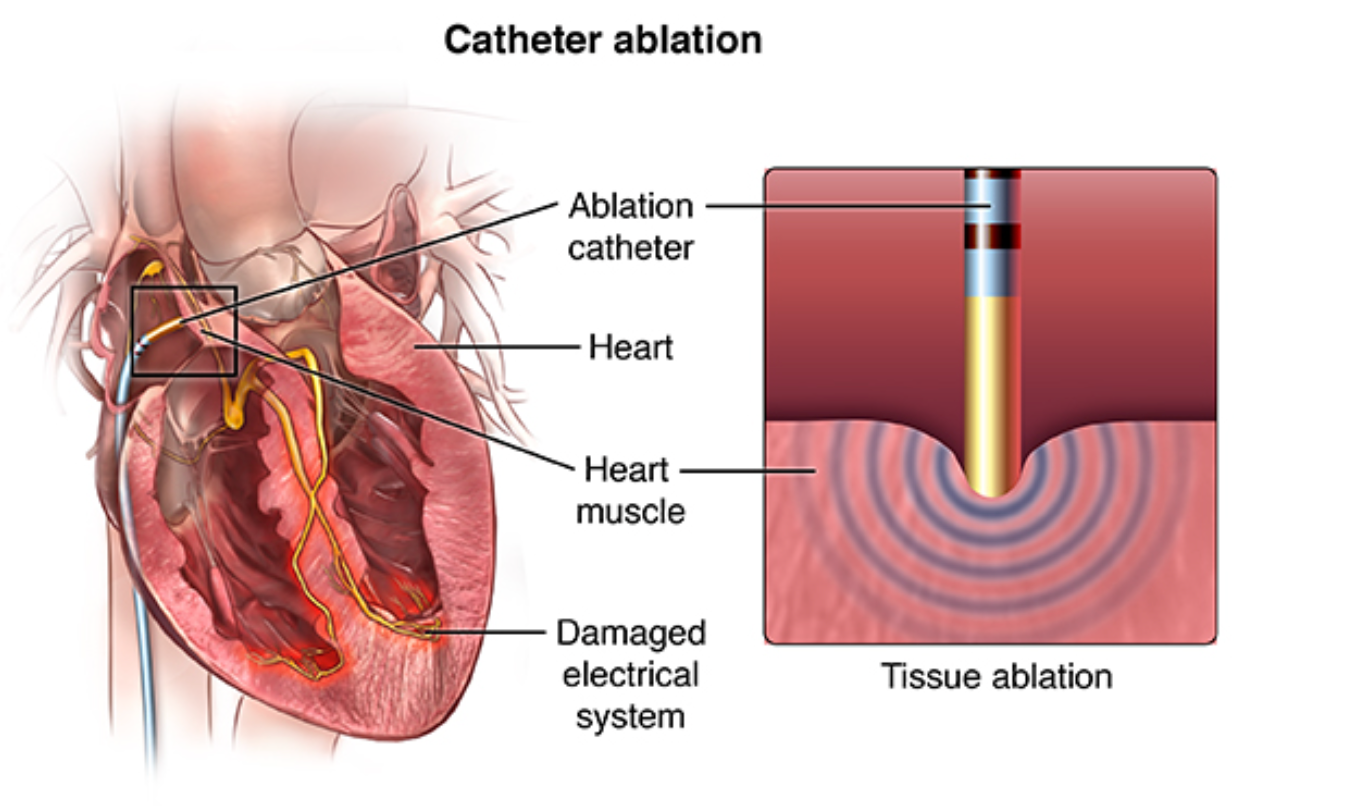
Background: Patients with advanced end-stage heart failure often require heart transplantation or left ventricular assist device implantation for favorable outcomes. This study explores the effectiveness of catheter ablation in improving outcomes for heart failure patients with symptomatic atrial fibrillation.
Summary: The CASTLE-HTx trial investigated the safety and efficacy of catheter ablation in patients with end-stage heart failure and symptomatic atrial fibrillation. The primary endpoint was a composite of death, left ventricular assist device implantation, or urgent heart transplantation. The trial demonstrated that catheter ablation combined with medical therapy significantly reduced this primary endpoint compared to medical therapy alone.
Endpoints:
- Primary Endpoint: Composite of death, left ventricular assist device implantation, or urgent heart transplantation.
- Secondary Endpoints: Death from cardiovascular causes, left ventricular ejection fraction, and atrial fibrillation burden at 6 and 12 months.
Statistical Analysis:
- The trial was designed with 80% power to detect a significant difference.
- The primary endpoint showed a hazard ratio of 0.24 with a 95% confidence interval (CI) of 0.11 to 0.52 (P<0.001).

What is hazard ratio?
A hazard ratio (HR) is a statistical measure used in survival analysis, particularly in medical research, to assess the relative risk of an event (such as death, disease recurrence, or treatment failure) between two groups. It quantifies the likelihood of an event occurring in one group compared to another over a specified period. An HR less than 1 indicates a reduced risk in the first group, while an HR greater than 1 suggests an increased risk, and an HR equal to 1 implies no difference in risk between the groups.
- Kaplan-Meier estimates revealed that the cumulative incidence of the primary endpoint at 1 and 2 years was 6% and 9%, respectively, in the ablation group and 28% and 31%, respectively, in the medical-therapy group.
What is Kaplan-Meier?
Kaplan-Meier is used to calculate the probability of an event (like patient survival or disease recurrence) over time. It creates a survival curve that shows how the probability of experiencing the event changes as time progresses. This curve is valuable for comparing different groups or treatments and is commonly used in studies related to patient outcomes and survival analysis.
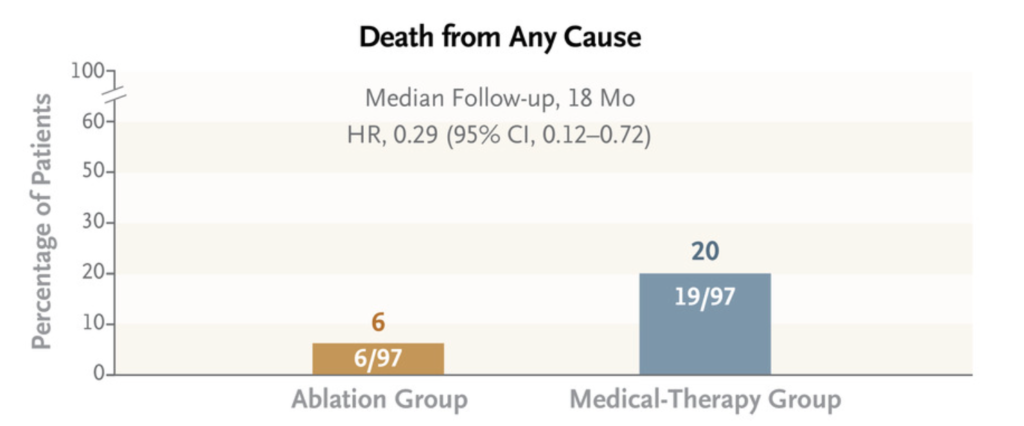
- Death from any cause occurred in 6% of patients in the ablation group and 20% in the medical-therapy group (hazard ratio 0.29, 95% CI 0.12 to 0.72).
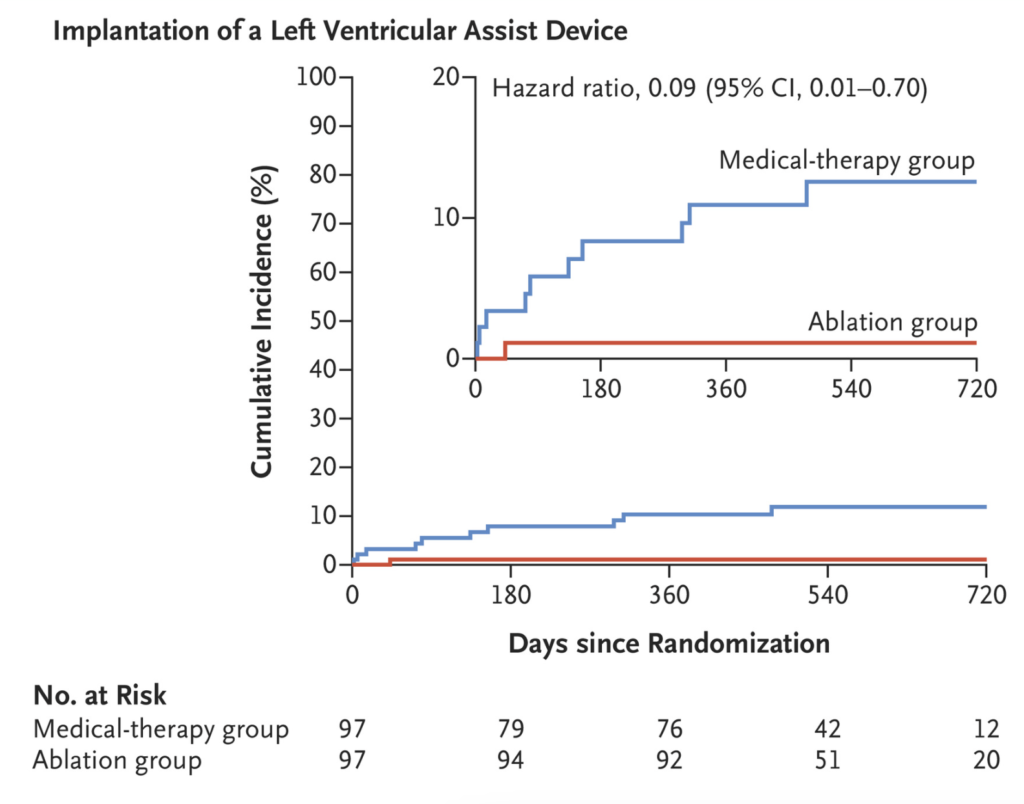
- Left ventricular assist device implantation occurred in 1% of patients in the ablation group and 10% in the medical-therapy group (cause-specific hazard ratio 0.09, 95% CI 0.01 to 0.70).
- Urgent heart transplantation was performed in 1% of patients in the ablation group and 6% in the medical-therapy group (cause-specific hazard ratio 0.15, 95% CI 0.02 to 1.25).
- Changes in left ventricular ejection fraction and atrial fibrillation burden were statistically significant between the ablation and medical-therapy groups at 6 and 12 months.
Critical Analysis: The CASTLE-HTx trial highlights the significant benefits of catheter ablation in patients with end-stage heart failure and atrial fibrillation. It suggests that catheter ablation can reduce arrhythmia burden, reverse left ventricular remodelling, and lower mortality in these patients. Importantly, the trial indicates that catheter ablation should not delay transplantation consideration.
Limitations:
- Single-Center Trial: The study was conducted at a single referral center, potentially limiting its generalizability.
- Early Termination: The trial was terminated early based on the recommendation of the data and safety monitoring board, and longer-term outcomes remain uncertain.
- Crossover Patients: Some patients in the medical-therapy group crossed over to undergo catheter ablation, potentially affecting the treatment benefit associated with ablation.
In conclusion, the CASTLE-HTx trial suggests that catheter ablation, when combined with medical therapy, can significantly improve outcomes for patients with end-stage heart failure and symptomatic atrial fibrillation. This approach may reduce the need for urgent interventions like heart transplantation or ventricular assist device implantation. However, the study’s limitations should be considered in interpreting these results.
The full Research paper can be found on NEJM.
Reference:
Diller, GP, Bruck, HA, Breithardt, G, et al. Catheter Ablation in End-Stage Heart Failure with Atrial Fibrillation. N Engl J Med. 2023 Oct 20;389(16):1485-1495. doi: 10.1056/NEJMoa2306037. Epub 2023 Sep 28.
Leave a Reply